
Creatine: A Comprehensive Guide
A guide to understanding the "King of Supplements"

What is creatine?
Creatine is a naturally occurring substance in the human body that is produced from the amino acids methionine, glycine, and arginine. It plays a role in the ATP phosphocreatine energy system, which provides energy for the initial 10 seconds of high-intensity activities. The body naturally synthesizes creatine, but it is also constantly broken down into creatinine. A diet containing one to two grams of creatine per day, typically found in meat, is sufficient to maintain muscle creatine levels for omnivores. Vegetarians have lower creatine levels compared to meat eaters and may benefit more from supplementation. Chronic supplementation of creatine has been shown to increase muscle creatine levels by about 30% in omnivores and to enhance strength, power, and hypertrophy [1].
The most common and recommended form of creatine is creatine monohydrate and no other forms have been proven to be superior. Creatine monohydrate is the most extensively studied and effective sports supplement. It is also one of the most popular supplements among athletes and fitness enthusiasts. Studies have consistently demonstrated that creatine supplementation increases the levels of creatine stored in the muscle, which is believed to contribute to the observed improvements in high-intensity exercise performance and increased training adaptations. Apart from athletic performance, research has also shown that creatine supplementation may support post-exercise recovery, injury prevention, thermoregulation, rehabilitation, and even protection against concussion and spinal cord injuries [1].

In this post, I will cover how creatine works, its safety profile, its ergogenic benefits, recommended dosage, creatine’s effect on recovery, other forms of creatine, as well how to make the best purchase when purchasing the supplement. Let’s get started.
How does creatine work?
Creatine phosphate, also known as phosphocreatine, is a molecule that plays a critical role in providing energy for high-intensity exercise. It works by donating a phosphate group to ADP (adenosine diphosphate) to form ATP (adenosine triphosphate), which is the primary energy currency of the body. During high-intensity exercise, such as weightlifting or sprinting, the body's demand for energy increases and the stores of phosphocreatine in the muscle are rapidly depleted. Simply stated, creatine provides your muscles with energy to do more work.


When creatine is ingested, it is converted into phosphocreatine and stored in the muscle tissue, ready to be used as a source of energy during high-intensity exercise. Creatine is found in small amounts in certain foods, such as meat and fish, but can also be obtained through supplementation. From a typical diet, 1-2 g of creatine are consumed per day resulting in our muscles being roughly 60-80% saturated. This leaves us with 20-40% creatine un-stored and needed to be supplemented.

Supplementing with creatine monohydrate increases muscle creatine stores to levels that are difficult to attain through diet alone. This increase in muscle creatine results in an ergogenic boost (improvement in athletic performance), as well as an increase in muscle mass over time due to the increased ability of the muscle to produce energy during high-intensity exercise, leading to greater training adaptations. Sounds great, but what is its safety profile?
Safety
Creatine has been the subject of over 1,000 studies and widely used since the 1990s. The only consistently reported side effect from its supplementation is weight gain with some rare side effects of gastrointestinal distress (stomach aches), especially for those taking doses higher than a maintenance dose of ~3-5g/day.
Studies on healthy and diseased populations ranging from infants to the elderly, and at dosages from 0.3 to 0.8 g/kg/day for up to 5 years have shown that creatine supplementation is safe and may provide health and performance benefits. Additionally, claims that creatine increases the risk of musculoskeletal injuries, dehydration, muscle cramping, or has long-term detrimental effects have been refuted by clinical studies.
Some studies suggest that individuals taking creatine with or without other supplements may present with high creatinine levels and renal dysfunction. However, many researchers have found that creatine supplementation does not negatively affect renal function in healthy or clinical populations. Studies on adolescents, younger, and older populations have reported ergogenic benefits with no significant side effects.
There is growing evidence of the potential medical uses of creatine supplementation to improve health and well-being as one ages or to provide therapeutic benefit in clinical populations. Some studies recommended that individuals should consume 3 g/day of creatine throughout their lifespan to promote general health.
Below is the official position of the international society of sports nutrition (learn more about the ISSN) on the safety of creatine [2].
Position of the international society of sports nutrition (ISSN)
After reviewing the scientific and medical literature in this area, the International Society of Sports Nutrition concludes the following in terms of creatine supplementation as the official Position of the Society:
1. Creatine monohydrate is the most effective ergogenic nutritional supplement currently available to athletes with the intent of increasing high-intensity exercise capacity and lean body mass during training.
2. Creatine monohydrate supplementation is not only safe, but has been reported to have a number of therapeutic benefits in healthy and diseased populations ranging from infants to the elderly. There is no compelling scientific evidence that the short- or long-term use of creatine monohydrate (up to 30 g/day for 5 years) has any detrimental effects on otherwise healthy individuals or among clinical populations who may benefit from creatine supplementation.
3. If proper precautions and supervision are provided, creatine monohydrate supplementation in children and adolescent athletes is acceptable and may provide a nutritional alternative with a favorable safety profile to potentially dangerous anabolic androgenic drugs. However, we recommend that creatine supplementation only be considered for use by younger athletes who: a.) are involved in serious/competitive supervised training; b.) are consuming a well-balanced and performance enhancing diet; c.) are knowledgeable about appropriate use of creatine; and d.) do not exceed recommended dosages.
4. Label advisories on creatine products that caution against usage by those under 18 years old, while perhaps intended to insulate their manufacturers from legal liability, are likely unnecessary given the science supporting creatine’s safety, including in children and adolescents.
5. At present, creatine monohydrate is the most extensively studied and clinically effective form of creatine for use in nutritional supplements in terms of muscle uptake and ability to increase high-intensity exercise capacity.
6. The addition of carbohydrate or carbohydrate and protein to a creatine supplement appears to increase muscular uptake of creatine, although the effect on performance measures may not be greater than using creatine monohydrate alone.
7. The quickest method of increasing muscle creatine stores may be to consume ~0.3 g/kg/day of creatine monohydrate for 5–7-days followed by 3–5 g/day thereafter to maintain elevated stores. Initially, ingesting smaller amounts of creatine monohydrate (e.g., 3–5 g/day) will increase muscle creatine stores over a 3–4 week period, however, the initial performance effects of this method of supplementation are less supported.
8. Clinical populations have been supplemented with high levels of creatine monohydrate (0.3 – 0.8 g/kg/day equivalent to 21–56 g/day for a 70 kg individual) for years with no clinically significant or serious adverse events.
9. Further research is warranted to examine the potential medical benefits of creatine monohydrate and precursors like guanidinoacetic acid on sport, health and medicine.
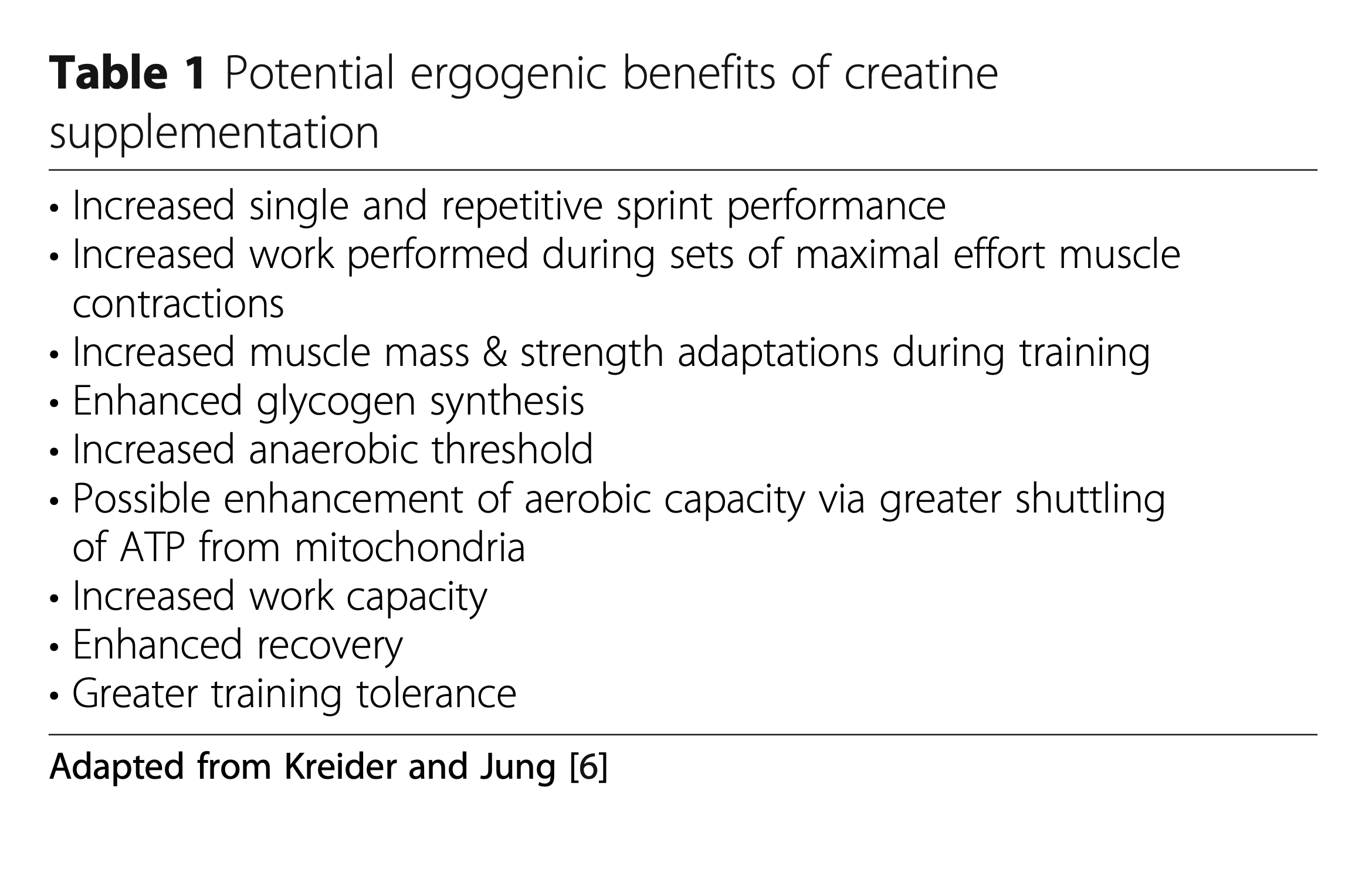
Ergogenic benefits
Creatine supplementation has been extensively studied and a large body of evidence now supports its effectiveness in enhancing exercise capacity and training adaptations in athletes and individuals of various ages. By increasing the muscle's availability of creatine and PCr, individuals can experience better acute exercise performance and improved training adaptations. This can lead to greater gains in strength, muscle mass, and overall performance, making it an effective ergogenic aid for power/strength athletes and those involved in high-intensity sports.
Studies have shown that after creatine loading (we will touch on this in the next section), high-intensity and repetitive exercise performance can improve by 10-20%. While the majority of studies have been conducted on men, benefits have also been reported in women, although some studies suggest women may not see as much gain in strength and muscle mass.
The scientific community has reached a wide-spread consensus on the effectiveness of creatine supplementation as a nutritional aid for athletes. This is reflected in position stands by organizations such as the International Society of Sports Nutrition, American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine, which have all concluded that creatine monohydrate is the most effective ergogenic supplement currently available for athletes in terms of increasing high-intensity exercise capacity and lean body mass during training.
Recommended Dosing & Creatine Loading
Creatine requires time to become saturated in the muscles. This can take anywhere from a week to a month depending on the approach. There are two paths you can take.

Method 1: Creatine loading
This method, which consists of consuming four doses per day over the course of 5-7 days, for a total of a total of 20g of creatine, has been a strategy of reaching maximal saturation of muscle creatine the fastest. Afterward, 3-5g/day for maintenance and for larger athletes, 5-10g/day. With this approach, you can expect a more steep weight gain due to the retention of water in the muscles but also run the risk of some minor side effects. The most common is that of gastrointestinal distress (more commonly known as a stomach ache).Method 2: Maintenance approach
For a more gradual increase in muscle creatine, ingesting the maintenance dosage of 3-5g/day for 28 days to reach maximal saturation of the muscle. This is beneficial and recommended for those who are cutting and want to slowly offset the weight gain due to the retention of water in the muscles. It is also likely to reduce the chance of gastrointestinal distress.Method 3: Middle Ground Approach
It’s common to think of creatine loading as a dichotomy when in reality there is a spectrum of approaches one can take between 3-20g/day to reach maximal starvation of the muscle. 10g/day (two 5g doses a day) for two weeks is another viable approach which lightens the loading phase for double the time (1 to 2 weeks) — that is, if you believe in loading at all…
Recent developments on the skepticism behind creatine loading
While important research into the topic of fast-tracking creatine loading into the muscle has been done(4), the study was done with a 3g/day maintenance approach (as discussed in Method 2) vs. a 40% increased daily dose of 5g/day. Recent studies [5] using the 5g/day method of maintenance found similar increases (~24%) in muscle creatine content after 14 days, the same as a 6-day, 20g per day loading protocol as discussed in Method 1 above.
Enhanced Recovery
Creatine supplementation has been shown to be beneficial in promoting recovery for athletes who undergo intense training. Several studies have reported the positive effects of creatine supplementation on muscle recovery and performance.
Green and coworkers [6] showed that ingesting creatine (5 g) along with glucose (95 g) improved the storage of both creatine and carbohydrates in the muscles. Similarly, Steenge et al. [7] reported that co-ingesting creatine (5 g) with carbohydrates (47-97 g) and protein (50 g) enhanced creatine retention in the muscles.
Nelson and colleagues [8] showed that creatine supplementation along with glycogen loading prior to an exhaustive exercise bout was more effective in restoring glycogen levels compared to carbohydrate loading alone. Glycogen replenishment is important in preventing overtraining during intense training periods, and thus creatine supplementation can help athletes maintain optimal glycogen levels during intensive training.
Cooke and associates [9] evaluated the effects of creatine supplementation on muscle force recovery and muscle damage following intense exercise and reported that participants who took creatine had greater isokinetic (+10%) and isometric (+21%) knee extension strength during recovery, and significantly lower plasma CK levels (−84%) compared to controls.
Santos and coworkers [10] found that creatine supplementation reduced changes in CK (−19%), prostaglandin E2 (−61%), TNF alpha (−34%), and abolished the increase in lactate dehydrogenase (LDH) in experienced marathon runners prior to a 30 km race. Demince et al. reported similar findings, with creatine supplementation inhibiting the increase of TNF-alpha and C-reactive protein in response to intermittent anaerobic sprint exercise.
Volek and colleagues [11] evaluated the effects of creatine supplementation (0.3 g/ kg/d) during an intensified overreaching period followed by a 2-week taper and found that creatine supplementation helped maintain muscular performance during high-volume resistance training, which otherwise leads to small performance decrements.
Overall, these findings suggest that creatine supplementation can help athletes enhance glycogen loading, reduce inflammation and muscle enzyme efflux following intense exercise, and tolerate high volumes of training, thereby promoting recovery.
Are other forms of creatine better than creatine monohydrate?
Creatine monohydrate is effective in increasing muscle creatine stores, leading to its ergogenic effects, and has a proven safety record. Therefore, it is recommended to stick with creatine monohydrate and avoid wasting money on alternative forms as there is no evidence to suggest that alternative forms of creatine are superior to creatine monohydrate. In fact, they have not been shown to offer any additional benefits and are often more expensive, costing 2-8 times more [12].

Due to the popularity of energy drinks, “Super Creatine” has been coined. A recent study [13] evaluated the effects of "Super Creatine®", also known as creatyl-L-leucine, as a novel form of creatine supplement. Results showed that creatyl-L-leucine failed to significantly increase muscle creatine levels compared to creatine monohydrate. There was a small increase in lean body mass in the creatine monohydrate group, while the placebo and creatyl-L-leucine groups showed no significant changes. The evidence is beginning to stack against alternative forms of creatine, which are more expensive but do not perform better than creatine monohydrate.

Concluding thoughts
Is creatine, and especially creatine monohydrate, the "king of supplements”? Creatine monohydrate has been widely studied and proven to be a safe and effective supplement for athletes and weight lifters looking to increase their performance and recovery. The body of evidence suggests that creatine supplementation can lead to significant improvements in strength, power, and muscle mass, making it a valuable tool for those looking to enhance their training results. While results will vary individual to individual, creatine has established itself as a reliable and effective supplement for athletes and fitness enthusiasts, earning, in our eyes and the eyes of many, the title of "king of supplements."
1 Kreider, R.B., Kalman, D.S., Antonio, J. et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr 14, 18 (2017). https://doi.org/10.1186/s12970-017-0173-z
2 Buford TW, Kreider RB, Stout JR, Greenwood M, Campbell B, Spano M, Ziegenfuss T, Lopez H, Landis J, Antonio J. International Society of Sports Nutrition position stand: creatine supplementation and exercise. J Int Soc Sports Nutr. 2007 Aug 30;4:6. doi: 10.1186/1550-2783-4-6. PMID: 17908288; PMCID: PMC2048496.
3 Rodriguez NR, DiMarco NM, Langley S; American Dietetic Association; Dietitians of Canada; American College of Sports Medicine: Nutrition and Athletic Performance. Position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J Am Diet Assoc. 2009 Mar;109(3):509-27. doi: 10.1016/j.jada.2009.01.005. Erratum in: J Am Diet Assoc. 2013 Dec;113(12):1759. PMID: 19278045.
4 Hultman E, Söderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol (1985). 1996 Jul;81(1):232-7. doi: 10.1152/jappl.1996.81.1.232. PMID: 8828669.
5 Askow AT, Paulussen KJM, McKenna CF, Salvador AF, Scaroni SE, Hamann JS, Ulanov AV, Li Z, Paluska SA, Beaudry KM, De Lisio M, Burd NA. Creatine Monohydrate Supplementation, but not Creatyl-L-Leucine, Increased Muscle Creatine Content in Healthy Young Adults: A Double-Blind Randomized Controlled Trial. Int J Sport Nutr Exerc Metab. 2022 Aug 25;32(6):446-452. doi: 10.1123/ijsnem.2022-0074. PMID: 36007881.
6 Green AL, et al. Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans. Am J Physiol. 1996;271(5 Pt 1):E821–6.
7 Steenge GR, Simpson EJ, Greenhaff PL. Protein- and carbohydrate-induced augmentation of whole body creatine retention in humans. J Appl Physiol (1985). 2000 Sep;89(3):1165-71. doi: 10.1152/jappl.2000.89.3.1165. PMID: 10956365.
8 Nelson AG, Arnall DA, Kokkonen J, Day R, Evans J. Muscle glycogen supercompensation is enhanced by prior creatine supplementation. Med Sci Sports Exerc. 2001 Jul;33(7):1096-100. doi: 10.1097/00005768-200107000-00005. PMID: 11445755.
9 Cooke MB, Rybalka E, Williams AD, Cribb PJ, Hayes A. Creatine supplementation enhances muscle force recovery after eccentrically-induced muscle damage in healthy individuals. J Int Soc Sports Nutr. 2009 Jun 2;6:13. doi: 10.1186/1550-2783-6-13. PMID: 19490606; PMCID: PMC2697134.
10 Santos RV, Bassit RA, Caperuto EC, Costa Rosa LF. The effect of creatine supplementation upon inflammatory and muscle soreness markers after a 30km race. Life Sci. 2004 Sep 3;75(16):1917-24. doi: 10.1016/j.lfs.2003.11.036. PMID: 15306159.
11 Volek JS, Ratamess NA, Rubin MR, Gómez AL, French DN, McGuigan MM, Scheett TP, Sharman MJ, Häkkinen K, Kraemer WJ. The effects of creatine supplementation on muscular performance and body composition responses to short-term resistance training overreaching. Eur J Appl Physiol. 2004 May;91(5-6):628-37. doi: 10.1007/s00421-003-1031-z. Epub 2003 Dec 18. PMID: 14685870.
12 Fazio, Carly1; Elder, Craig L.2; Harris, Margaret M.1. Efficacy of Alternative Forms of Creatine Supplementation on Improving Performance and Body Composition in Healthy Subjects: A Systematic Review. Journal of Strength and Conditioning Research ():, February 11, 2021. | DOI: 10.1519/JSC.0000000000003873
13 Askow AT, Paulussen KJM, McKenna CF, Salvador AF, Scaroni SE, Hamann JS, Ulanov AV, Li Z, Paluska SA, Beaudry KM, De Lisio M, Burd NA. Creatine Monohydrate Supplementation, but not Creatyl-L-Leucine, Increased Muscle Creatine Content in Healthy Young Adults: A Double-Blind Randomized Controlled Trial. Int J Sport Nutr Exerc Metab. 2022 Aug 25;32(6):446-452. doi: 10.1123/ijsnem.2022-0074. PMID: 36007881.
Any product recommendations? I'm looking to start trying the maintenance approach.